Best Medical Coding Institute and Training center in Trivandrum
N25.0
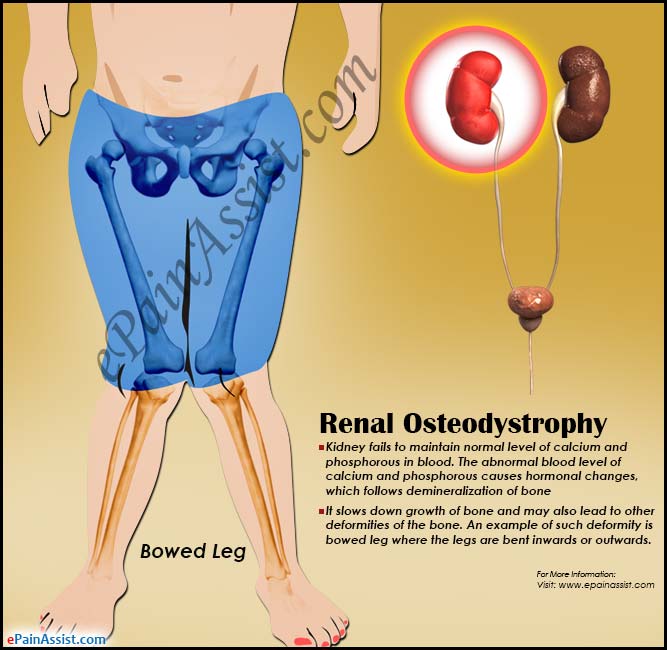
Renal Osteodystrophy
Renal osteodystrophy is one of the main complications of end-stage renal disease that leads to skeletal and extraskeletal manifestations. Although it may be unavoidable in patients undergoing hemodialysis, appropriate and timely interventions can help alleviate the symptoms experienced by the patients and also reduce the osteodystrophy-related comorbidities. This activity reviews the evaluation and management of renal osteodystrophy and explains the role of the interprofessional team in improving the care of patients with this condition.
Objectives:
- Identify the etiology of renal osteodystrophy.
- Outline the physical findings of a patient with renal osteodystrophy.
- Describe the management considerations for patients with renal osteodystrophy.
- Summarize the importance of improving care coordination amongst the interprofessional team to improve outcomes for patients affected by renal osteodystrophy.
Renal osteodystrophy is a broad term that incorporates all the biochemical abnormalities and skeletal manifestations in patients suffering from chronic kidney disease or end-stage renal disease. The derangements in the serum levels of calcium, phosphorous, PTH, vitamin D, along with their effects on bone turnover, mineralization, and extraskeletal calcifications, are all important components of this condition. Reports suggest these abnormalities are most likely to be seen at a GFR below 60 mL/min/1.73 m2.
- The histopathological findings of renal osteodystrophy are commonly used to further classify this condition into:
Low bone turnover states, such as adynamic bone disease or heavy metal-induced osteomalacia
- The development of renal osteodystrophy as a complication of end-stage renal disease has also influenced changes in the treatment protocols and dialysis regimens in patients.

Osteomalacia is characterized by incomplete mineralization of normal osteoid tissue following closure of the growth plates. Osteomalacia may be part of the spectrum of osseous abnormalities that can be observed in patients with chronic renal insufficiency. This condition is referred to as renal osteodystrophy. Renal osteodystrophy combines features of secondary hyperparathyroidism, rickets, osteomalacia, and osteoporosis. Findings of rickets and osteomalacia occur in children, and findings of osteomalacia and secondary hyperparathyroidism occur in adults.
Clinically, osteomalacia is subtler than rickets, particularly in mild or moderate disease. Mildly affected patients may present with nonspecific bone pain and tenderness and possibly hypotoniaRenal osteodystrophy is invariably seen in patients of chronic kidney disease, although the disease processes may differ in patients. Histologically, there is a classification into high or low bone turnover states.
High bone turnover states: They lead to increased rates of bone resorption and formation. Increased parathyroid hormone (PTH) levels play a major role in the pathogenesis of high bone turnover states. Hyperparathyroidism can be primary, secondary, or tertiary. Neoplasms of the parathyroid glands secreting PTH autonomously, an example of tertiary hyperparathyroidism, can lead to a high bone turnover state.
Secondary hyperparathyroidism is the predominant cause of osteodystrophy. The different factors involved in the pathway building up to secondary hyperparathyroidism are also worth mentioning in the etiology of renal osteodystrophy:
- Phosphate retention: High phosphate levels in the blood can stimulate PTH secretion in more ways than one. It can either directly increase PTH mRNA levels or decrease the levels of calcium and calcitriol, indirectly causing a surge in PTH levels.
- Calcium: The relationship between calcium and PTH levels is well established. A decrease in serum calcium will also stimulate PTH secretion.
- Role of calcitriol: Calcitriol and PTH both increase serum calcium levels, and in cases of decreased calcitriol in the body, secondary hyperparathyroidism ensues due to decreased calcium absorption through the intestine and a reflex increase in PTH. Calcitriol is also required for suppressing PTH secretion by the parathyroid glands.
- Fibroblast growth factor 23: FGF-23 is responsible for decreasing phosphate levels in the body, and a decrease in FGF-23 can lead to secondary hyperparathyroidism.
The predominant histological bone pattern in renal osteodystrophy is osteitis fibrosa, which is a product of high bone turnover due to secondary hyperparathyroidism. Along with the PTH level, secondary factors that play a role in the development of osteitis fibrosa include interleukins 1, 6, and TNF-alpha.

Low bone turnover states: Diseases included here are mainly osteomalacia and dynamic bone disease, both seen in patients with end-stage renal disease (ESRD). The important factors that play a role in the pathogenesis are:
Osteomalacia: Heavy metal intoxication, mainly aluminum, can lead to dysfunction of both osteoblasts and osteoclasts. A defect in bone mineralization due to the dysfunctional osteoblast leads to an excess of accumulated bone matrix. Other metals implicated include iron and cadmium.
Adynamic bone disease (ABD): The pathogenesis of adynamic bone disease mainly revolves around the suppression of PTH, leading to low bone turnover and inadequate bone mineralization but no accumulation of excess osteoid in contrast to osteomalacia. Factors which lead to this include:
- Calcium and vitamin D: Aggressive treatment with these in patients of chronic kidney disease (CKD) causes a chronic suppression of PTH.
- Continuous ambulatory peritoneal dialysis (CAPD): This leads to a large influx of calcium into the body through the dialysate.
- Diabetes mellitus: Evidence suggests that elevated glucose and decreased insulin levels together suppress PTH secretion.
- Other factors: Interleukin 4 and a deficiency of osteogenic-protein 1 play secondary roles in the pathogenesis of ABD.
Mixed uremic osteodystrophy includes components of the high turnover osteitis fibrosa and low turnover mineralization defects, as seen in osteomalacia
National Institute of Medical Coding


Comments
Post a Comment